

Abstract
[Introduction]
Infant AML has been defined as AML in patients aged <1 year. Infant AML is related to high frequencies of M4, M5, and M7 subtypes in the FAB classification. Molecular analyses showed that KMT2A rearrangement (KMT2A-R), CBFA2T3-GLIS2 and NUP98-KDM5A are the most frequent abnormalities in infant AML. These findings indicate a distinct biology of infant AML. However, a more clinically adequate definition of "infant AML" by age remains controversial; a recent report by the COG defined patients aged <3 years with AML as infants because of their molecular similarities. Moreover, although Infants with AML are generally treated with dose-reduced regimens to avoid severe toxicities, it remains unknown whether patients aged 1-<3 years also require the same dose-reduced regimens as infants. Thus, further identification of AML in young pediatric patients is necessary.
[Methods]
This study enrolled patients aged <18 years who were diagnosed with de novo AML and who had participated in one of the two recent clinical trials in Japan: the AML99 trial and the AML-05 trial conducted by the Japanese Pediatric Leukemia/Lymphoma Study Group. In total, 723 patients were analyzed in the current study. Among them, bone marrow samples of 503 patients (70%) were screened for fusion genes and gene mutations.
[Results]
We first analyzed the distribution of fusion genes and FAB classification in 503 patients with clinical samples. Fusion genes were found in >50% of the patients in each age group. RUNX1-RUNX1T1, KMT2A-R, and CBFB-MYH11 were present in almost all age groups. RUNX1-RUNX1T1 was the most frequently identified fusion gene in all age groups excluding those <3 years, whereas KMT2A-R was the most frequently identified fusion gene in patients aged <3 years. Regarding other fusions, CBFA2T3-GLIS2 and NUP98-KDM5A were essentially limited to patients aged <3 years, whereas CBFB-MYH11 was detected in nearly all age groups. In the assessment of FAB classification, patients with M4 and M5 accounted for 50% of patients aged <3 years. Among patients aged <3 years, M7 was the second most common morphology. In total, approximately 80% of patients aged <3 years were classified as M4, M5, or M7. Conversely, M1 and M2, both of which display granulocytic differentiation, were the most frequent phenotypes among patients aged 3-<18 years. According to the distribution of fusion genes and FAB classification, we divided pediatric AML patients into two age groups: patients aged <3 years (patients <3y) and those aged 3-<18 years (patients 3-<18y). Further, we compared the prognostic effect of molecular characteristics between these two age groups, and identified KMT2A-R and CBFB-MYH11 as age-specific prognostic markers.
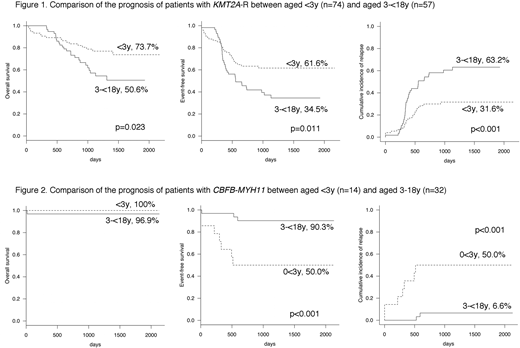
Furthermore, we analyzed the prognosis of KMT2A-R and CBFB-MYH11 in all 723 patients and confirmed that these fusions had significantly different prognoses between patients<3y and those 3-<18y. In the subgroup of patients with KMT2A-R (n = 131), 5-year (5y) OS, EFS, and CIR were significantly worse in patients 3-<18y (n = 57) than in patients <3y (n = 74) (50.6% vs 73.7%, p = 0.023; 34.5% vs 61.6%, p = 0.011; and 63.2% vs 31.6%, p <0.001, respectively) (Figure 1). Conversely, in the subgroup of patients with CBFB-MYH11 (n = 46), 5y EFS and CIR were significantly worse in patients <3y (n = 14) than in patients 3-<18y (n = 32) (50.0% vs 90.3%, p<0.001 and 50.0% vs 6.6%, p <0.001, respectively) (Figure 2).
In patients with KMT2A-R (n = 131), no molecular markers were identified as prognostic markers in combination with age; however, high WBC counts were related to poor prognosis regardless of age. Particularly, among patients 3-<18y (n = 57), those with WBC counts >10,000/µL (n = 37) had a significantly poorer prognosis than those with WBC <10,000/µL (n = 20) (5y OS 31.0% vs 78.8%, p = 0.002; 5y EFS 22.1% vs 54.2%, p = 0.008; and 5y CIR 77.9% vs 40.4%, p = 0.005).
In patients with CBFB-MYH11 with clinical samples (n = 39), NRAS-mutated patients (n = 13) had significantly better 5y EFS and CIR than NRAS-wild-type patients (n = 26) (100% vs 60.5%, p = 0.012, and 0% vs 35.7%, respectively). Moreover, the combination of NRAS status with age identified the worst prognosis in NRAS-wild-type patients <3y (5y EFS 22.2% and 5y CIR 77.8%).
[Conclusions]
Although age has not been used for the risk stratification of recent pediatric AML clinical trials, it might be a useful prognostic maker of this disease in combination with some molecular makers.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal